![]() This is a good technique for cases, where the laceration of cornea is melting, and this does not seem possible to close the wound adequately with nylon sutures. This usually happens when patients delay visit to the hospital much.
This is a good technique for cases, where the laceration of cornea is melting, and this does not seem possible to close the wound adequately with nylon sutures. This usually happens when patients delay visit to the hospital much.
This unfortunate boy got bad corneal trauma in April 2017, and during revision under anesthesia it stroke me that I am not able to close the wound and seal the anterior chamber properly. Immediate action was to do a total conjunctivotenon’s flap with intention to salvage the eye at least, though not the vision. I did a couple of Gundersen’s horisontal total conjunctival flaps and find it a bit cumbersome. Technique, where you don’t care of button-holes, while you are dissecting tenon’s and not conjunctiva, suited the situation best. This is a classic Kuhnt’s style vertical total flap, but also including tenon’s, and not just conjunctiva.
It does not just make surgery faster, but also provides more opportunities to seal the anterior chamber in case of big melting hole. Tenonplasty accelerates wound healing and provides robust scarring, as recent paper states (PMID: 28612422). In future it allows anterior segment reconstruction with corneal grafts and possible cataract surgery.
Tarsorrhaphy for two weeks helps a lot to preserve the flap in place.
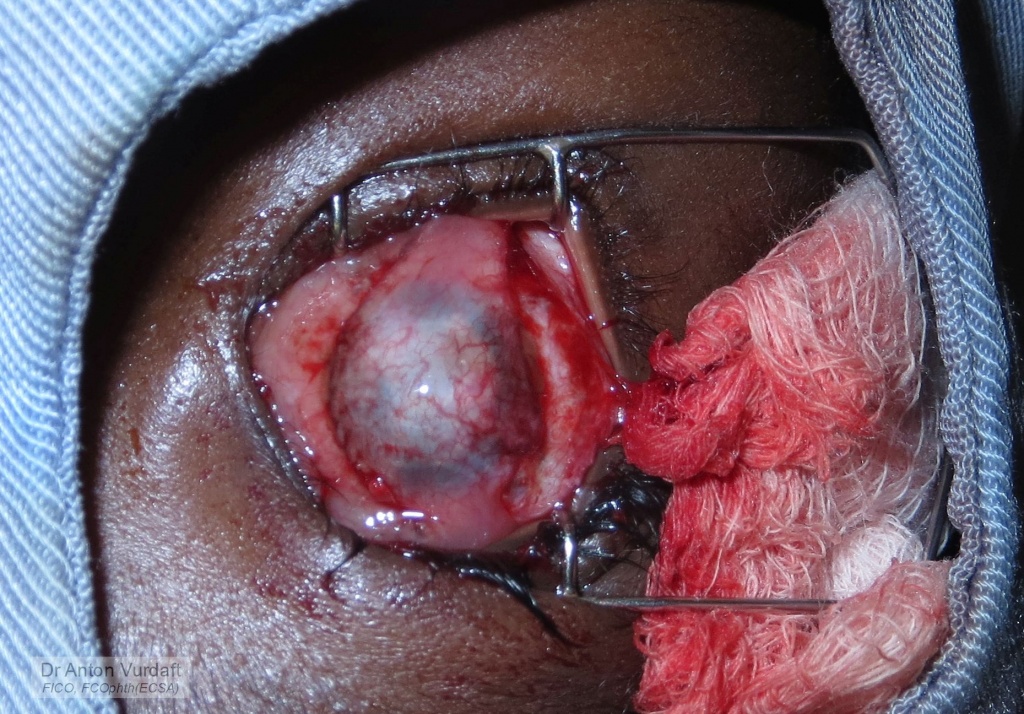
Total conjunctivotenon’s flap for corneal melted laceration. Intraoperative picture.

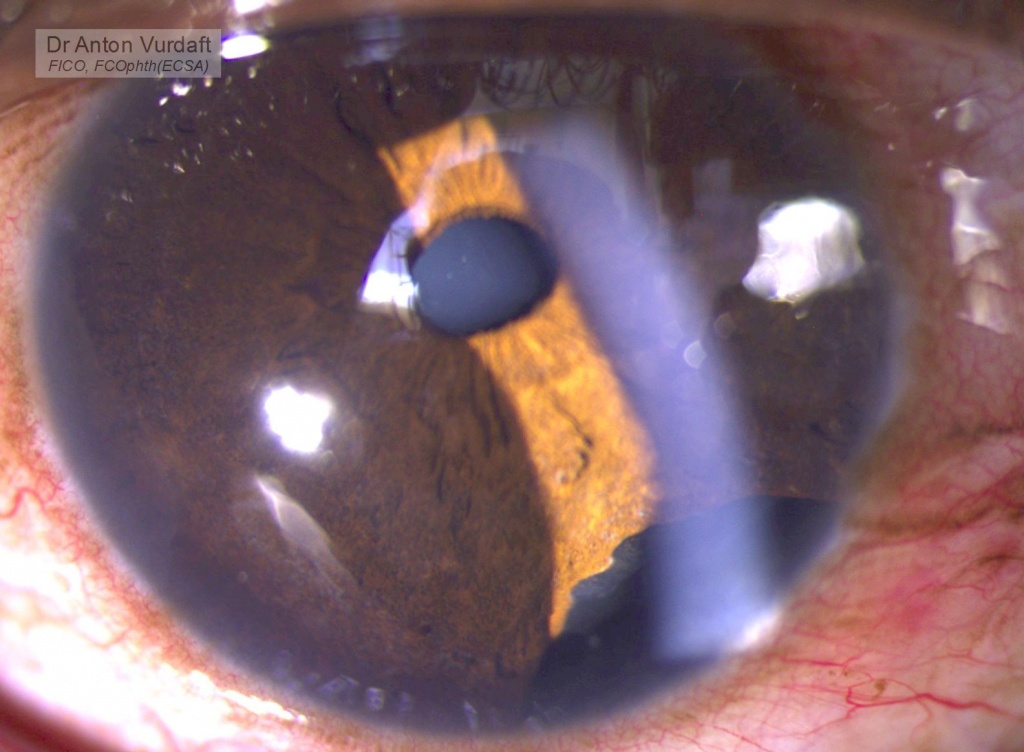
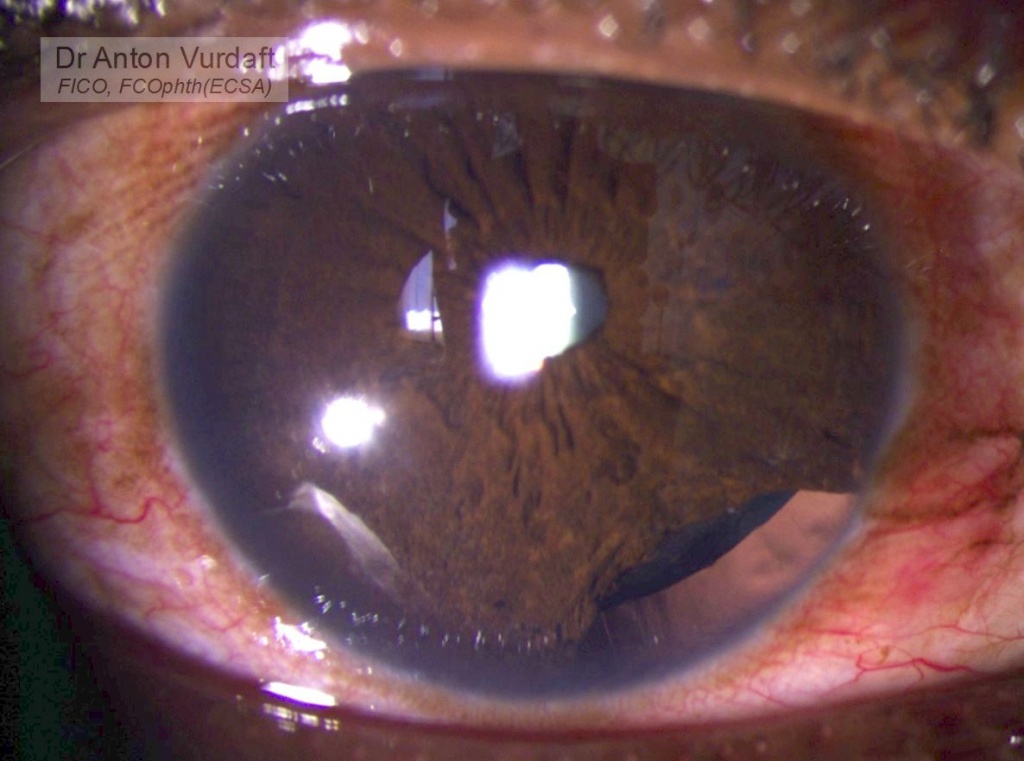
Total conjunctivotenon’s flap for melting corneal laceration. Postop status 3 months.