In the western world it is rare, to miss an OSSN and excise it as pterigium without no-touch technique etc. In one retrospective study from the US it was only in 0,3% of all cases of pterygium excision.
In tropical Africa, such cases are much more often. And vice versa, it is also commom to see a very suspective pterygium, that upon pathology proves to be benign… See this: Case 1 and Case 2
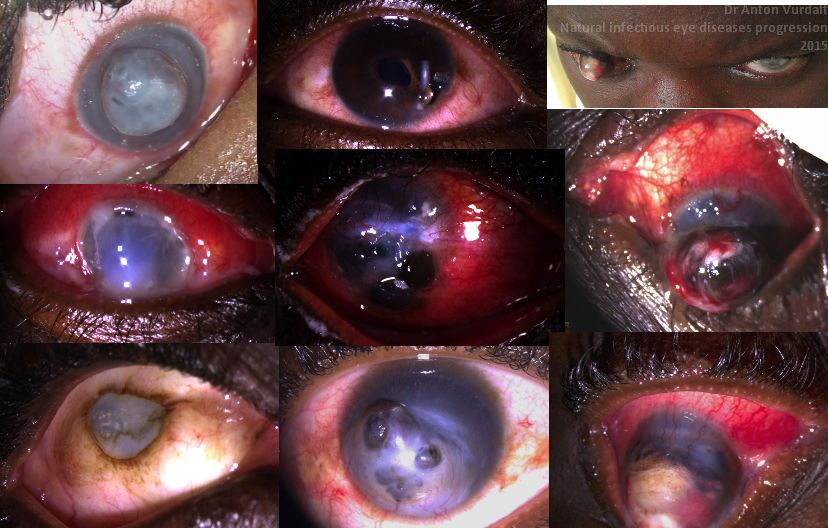
Cases of August 2015. Various variants of anterior staphylomas, often as a result of a treatment performed by local healers (“witch doctors”). Most of them are results of corneal ulcers.
anterior staphylomas
Сборник. “Глаза, проигранные природой”, про естественное течение инфекций глаза, подкреплённое иногда лечением от целителей. Эмоксипина и тауфона у целителей нет, но есть травки со схожим смыслом.
Уверенно этиологию могу сказать пожалуй что только на среднем фото первого столбца и первом фото второго столбца – гонококк. Остальное – из тех случаев, когда этиология уже не принципиальна. Травы от разного рода шаманов часто – основная этиология при незначительных до их применения кератитах.
Немного про передние стафиломы (как редкое явление в современной офтальмологии).
Фиброзная капсула глаза (роговицы и склера) – прочный каркас, который удерживает в равновесии всё содержимое яблока. При декомпенсации каркаса спереди (самое уязвимое место глаза) равновесие нарушается, и за счёт внутриглазного давления содержимое глазного яблока устремляется туда, где меньше сопротивления – на волю. Есть разные стадии стафилом – некоторые потенциально могут зарубцеваться, сохранив глаз как орган, а то и с хорошей перспективой по зрению (в случае пересадки роговицы). Если рубцевания на этой стадии не случилось, то радужка, хрусталик, а иногда ресничное тело и сетчатка со стекловидным телом – проваливаются в переднюю дырку и таким образом её тампонируют. В принципе природа и тут справляется, заставляя всё это рубцеваться, одна незадача – пациенту при этом больно. Я не знаю, что пациенты делают с этим, когда врача рядом нет. Но когда такой имеется – они приходят за помощью, как правило понимая, что их ожидает. Некоторые хватают ибупрофен и убегают насовсем, но большинство возвращаются на эвисцерацию (удаление всех внутренностей яблока и сохранение фиброзного каркаса). Боль проходит, появляется возможность использования протеза, восстановления эстетики. Другая категория (при маленьких стафиломах) при наличии других опций – выбирает другие. А это в основном – конъюнктивальные лоскуты, покрывающие стафилому и способствующие более быстрому рубцеванию.
Занятие при стафиломах не очень удачное, т.к. некоторые стафиломы прогрессируют даже после удачной конъюнктивальной пластики.
Manual small incision cataract surgery (MSICS) is a gold standard for high-volume cataract services in developing countries. Since recently (with the rise of global ophthalmology concept) it has become part of the best ophthalmology training programs in the US and across the world. It is an absolutely brilliant and gentle technique, which is especially suited for premature, mature and hypermature cataracts, as well as traumatic and congenital cataracts. But one can also apply the same technique to operate on immature cataracts. Here it won’t be so fast, as the aspiration of sticky cortex will take its time with Simcoe cannula. Nevertheless, all the stages are doable.
There are differences in capsulotomy diameter, which one needs for “normal” immature cataracts (~5-6 mm) and for hypermature cataracts (up to 9-10 mm!). In mature cataracts one has to use a dye (trypan blue), but also often to carefully decompress an elevated intralenticular pressure (which often fails and leads to capsular tear and/or “argentinian flag”-style tears)! This makes capsulotomy (and capsulorhexis as one of them) in mature cataracts more complex if compared to the one in immature “transparent” cataracts.
For MSICS I personally preferred mainly a so-called “can-opener” type of capsulotomy, as it is a) easier, b) faster, and c) safer. Once I had realized these benefits, I switched to this technique almost invariably. Can-opener is best for big mature nuclei and also for Morgagnian cataracts. I am, however, aware, that can-opener is almost always not a good option for phaco. At the same time I found continuous curvilinear capsulorhexis (CCC) technique in transparent (immature) cataracts pretty easy to perform in comparison to intumescent hypermature cataracts. However, CCC is also possible by MSICS on mature cataracts. One can do it through both a tunnel or a paracentesis. A tunnel offers greater maneuverability, a paracentesis offers more stable anterior chamber.
For CCC in MSICS one can employ a) insuline syringe needle, b) Utrata forceps (gives the best control over rhexis!) and c) McPherson tying forceps. The latter is non-toothed and is a sort of improvisation, when the correct forceps is inavailable (often the case in Tropics!). In this video I depicted typical variants of CCC by mature and hypermature (and intumescent and Morgagnian!) cataracts, both uncomplicated and complicated cases. The can-opener technique is presented in two cases here and also in the other video of this channel.
* Some of the videos were screened at the earlier stage of my MSICS career. Some of the capsulotomies depicted here could have been managed better, and do not necessarily represent the best possible surgical technique. After I had bought Utrata capsulorhexis-forceps during my trip to the USA in early 2017, I never used McPherson for this purpose anymore. So, I highly recommend to purchase Utrata early in your MSICS career. The video will however be a good one for the MSICS beginners in the tropics, who often have to tackle the complex intumescent lenses with suboptimal instruments, and who still have the right to do mistakes 🙂 I would anyways appreciate your (also critical) comments.
Those of you, who just start with MSICS – Keep it up!
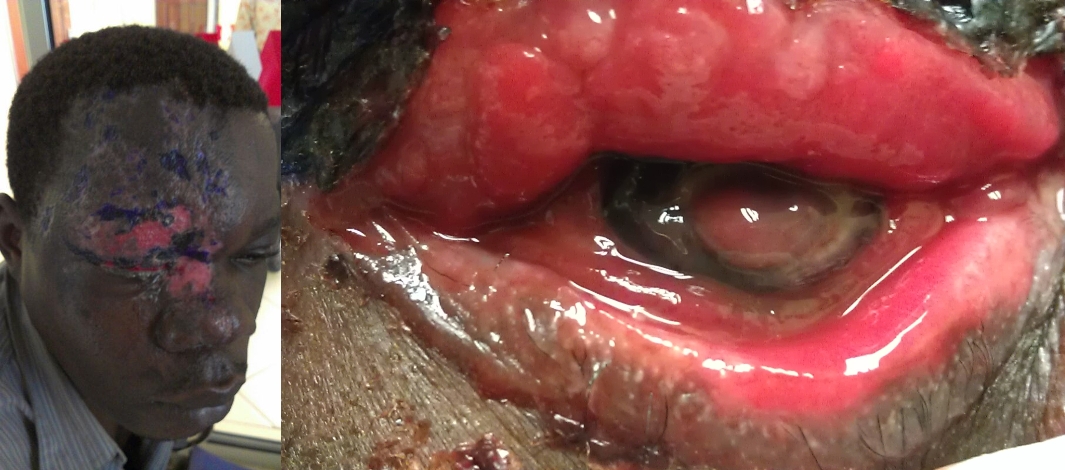
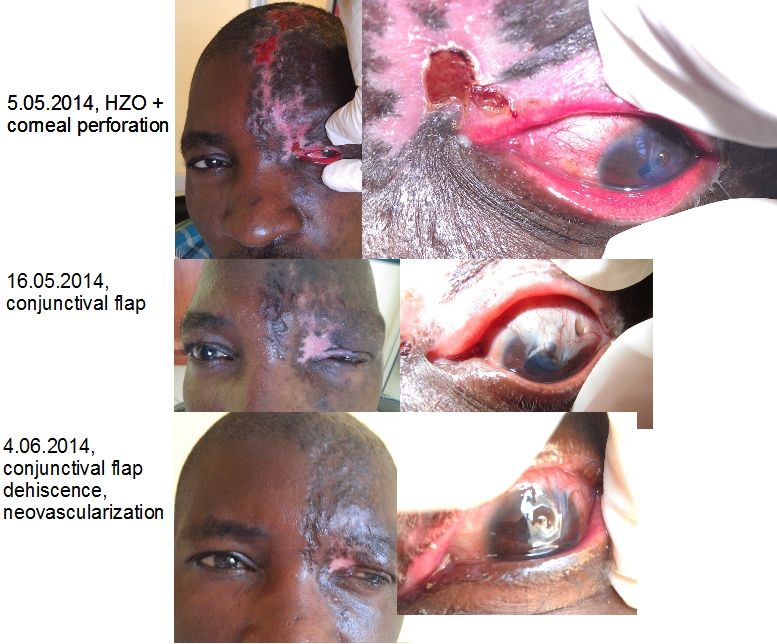
Herpes zoster ophthalmicus involves V1 cranial nerve (n.ophthalmicus). Here are three examples of herpes zoster in 2 young men and one 7yo girl. Both men are HIV-positive (this must be an AIDS-stage). HZO is definitely second quickest germ to penetrate and destroy the cornea. Pseudomonas has no chance in comparison to those two. HIV is certainly a boost for the fulminant clinic.
Герпес зостер c вовлечением первой ветви из моей африканской практики. Случай у двух взрослых мужчин и у девочки 7 лет (активный у мужчин, и в исходе у девочки). Herpes zoster ophthalmicus – наверное второй по скорости разъедания роговицы после гонококковой инфекции. Синегнойная палочка определённо нервно курит в сторонке. Мужчины были однозначно ВИЧ-положительны, а это, как известно, означает стадию СПИД. И это конечно одна из основных причин для такой яркой и драматической клинической картины.
Advanced herpes zoster ophthalmicus with corneal melt and lens/uvea prolapse. HIV positive patient.
Advanced herpes zoster ophthalmicus with resultant corneal leucoma in 7yo girl.
Advanced herpes zoster ophthalmicus with corneal melt and iris prolapse. HIV positive patient. Failed conjunctival flap adherence depicted.