This was a case of Mai 2016. Eleven y.o. boy came to our outpatient department with the father complaining of “growth” in one of boy’s eyes, that was allegedly present already for 2 weeks. Visual acuity 6/9 and there were no pains except photophobia. On examination – solid feathery cream-colored mass in the AC, adherant to the iris. Yellowish behind. No anterior chamber cells, no flare, absolutely quiet eye. Upon the HIV-test she was confirmed newly positive.
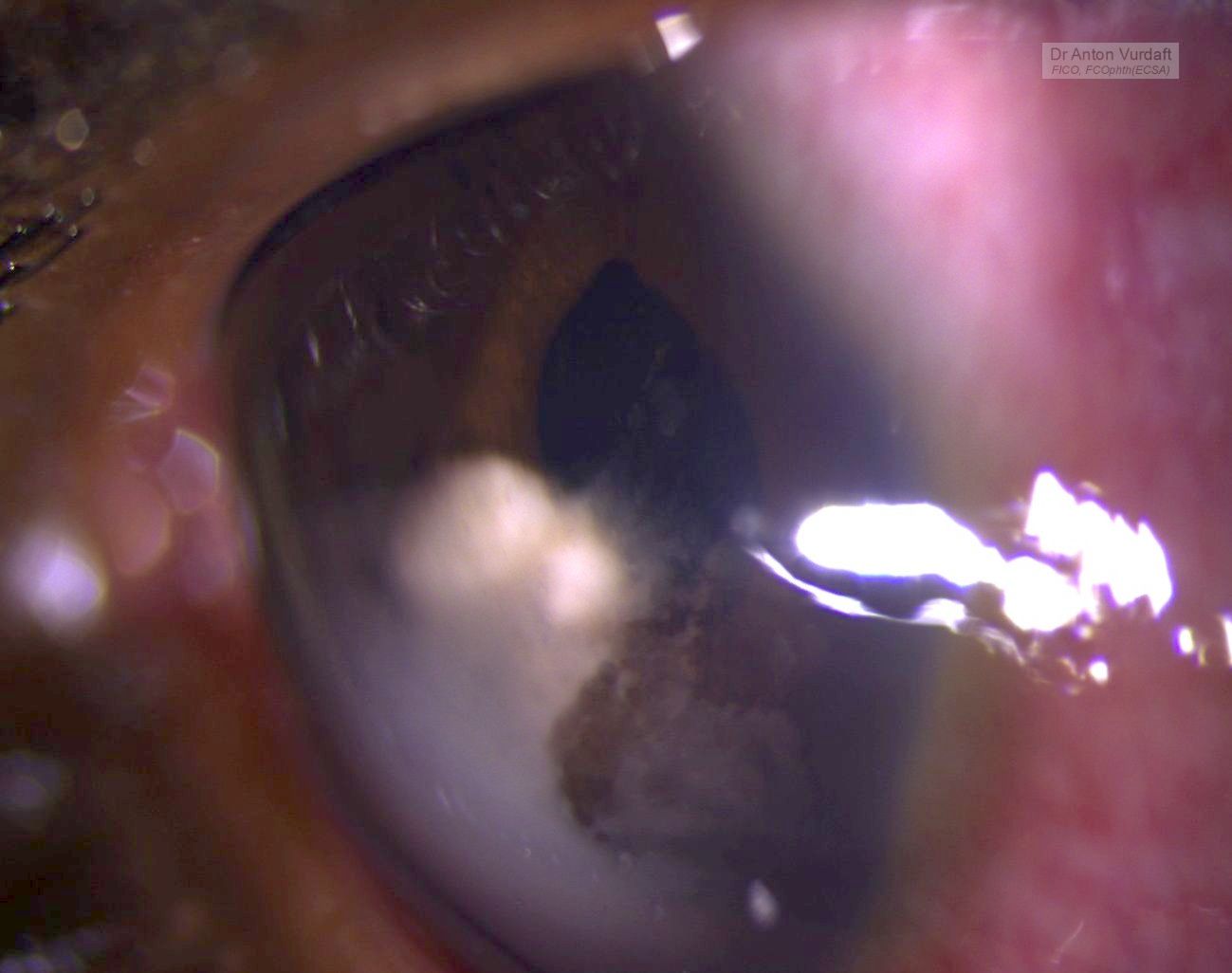
presumed aspergillosis iris-AC granuloma
presumed aspergillosis iris-AC granuloma
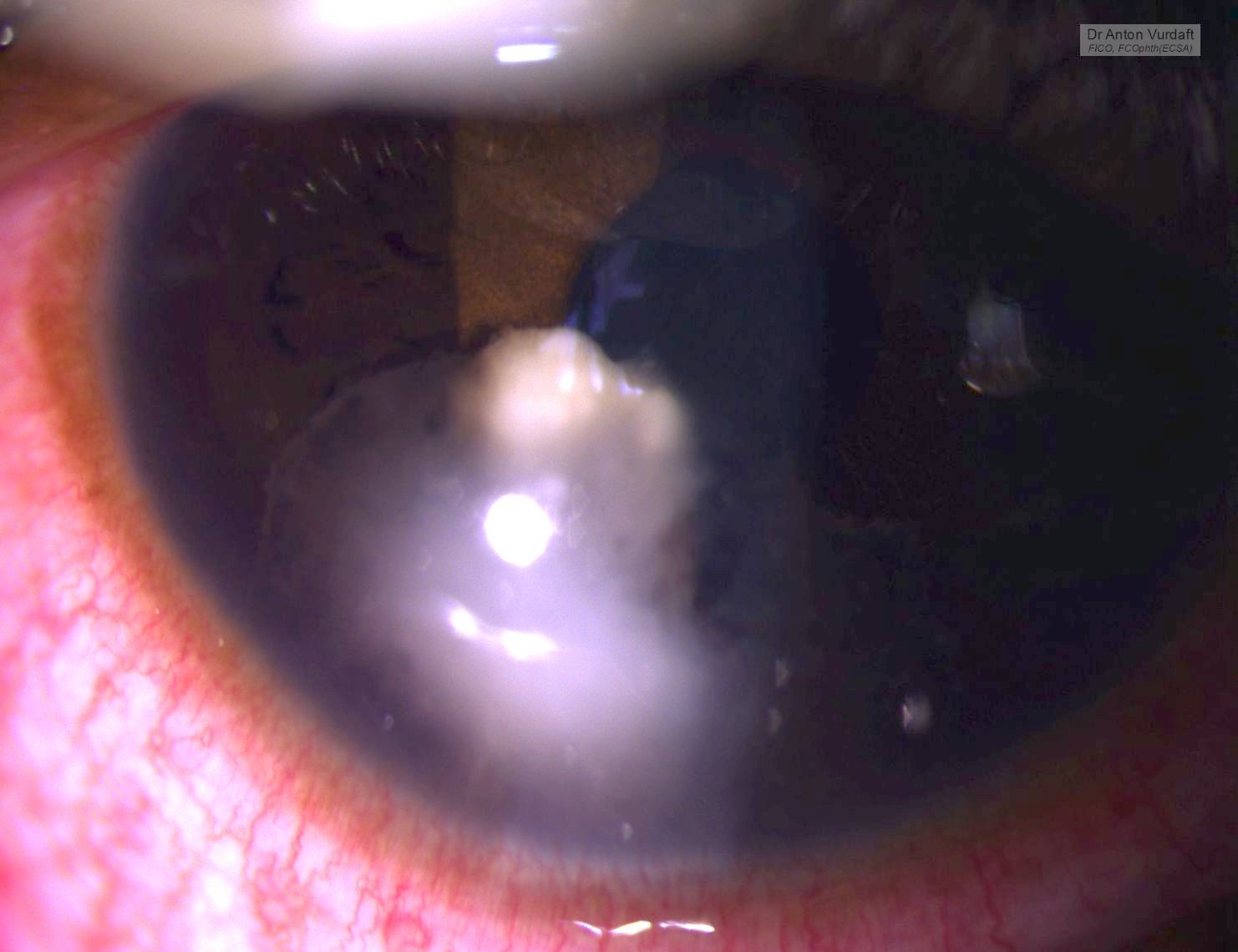
She was started on steroid and cycloplegic topical eye drops and NSAID tablets, and in 5 days the exudate was gone. But the iris cyst remained in place. There was no vitreous or retinal involvement, and the IOP was OK.

presumed aspergillosis iris-AC granuloma after tx, note torn posterior synechiae
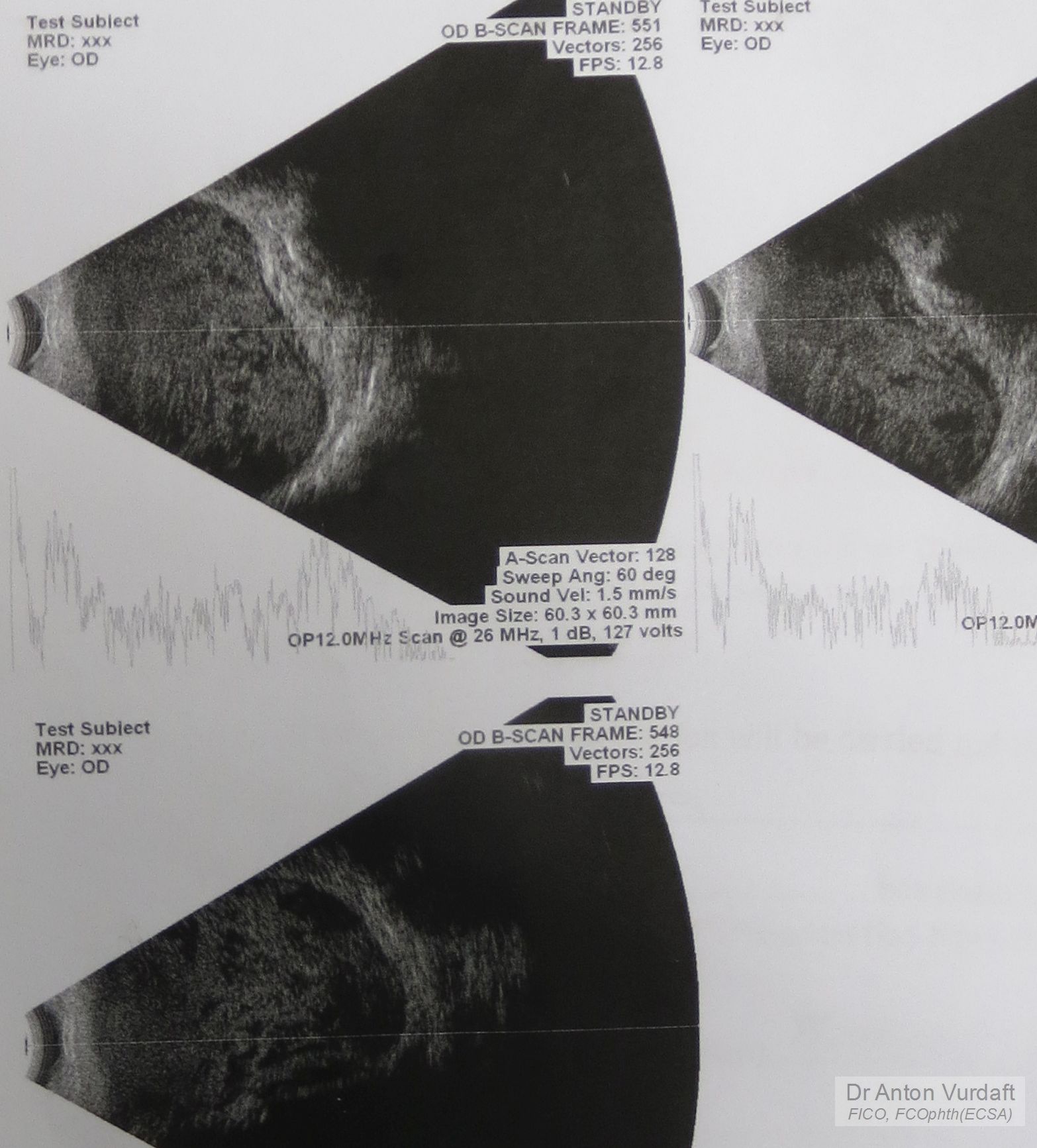
presumed aspergillosis iris-AC granuloma after tx: UBM-scan
Differential diagnosis: intraocular medulloepithelioma (must be congenital, but looks similar, although originating mostly from the angle or ciliary body, not the iris), intraocular lymphoma (looks simmilar, but much more scary!), tuberculoma, leproma, nonpigment melanoma or primary iris tumors, toxoplasmosis gumma, metastases in the iris (lungs, intestine, kidneys), fungi!
Other useful resources to review iris cysts:
eyewiki.aao.org/Iris_Cysts
bjo.bmj.com/content/59/5/276.full.pdf
https://www.archivesofpathology.org/doi/pdf/10.5858/arpa.2010-0669-RS
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3872564/
Literature search at that time in 2016 showed one paper from 2009 by Jain V with a similar case, Aspergillus iris granuloma: a case report with review of literature, claiming that to 2009 only three cases of aspergillosis of the anterior segment of the eye had been ever published. Here is a picture of their case:

Jain V, Aspergillus iris granuloma: a case report with review of literature. 2009
Our patient was left on the same topical treatment further in attempt to conquer the cyst and lost to follow-up. Unfortunately or fortunately, no iris-biopsy was performed that time, and therefore I had no microbiological evidence of fungi. One must also consider, that no natamycin was readily available topically in Western Province of Zambia that time, and in most of the times one must rely on antifungal activity of povidone-iodine eye drops (which are good and readily available hand made, by the way). One must strongly consider the lungs screening (CXR or CT) in immunocompromised patients, to exclude the primary source of hematogenous dissemination to
the brain or meninges. The immune status must be supported of course (f.e. HAART).
I thank my peer-colleagues from Terra-Ophthalmica for the kind help with the differential diagnosis and additional ideas for this case.







{kind=link}