Senanga town, Western Province of Zambia. April 2014.
Senanga, April 2014
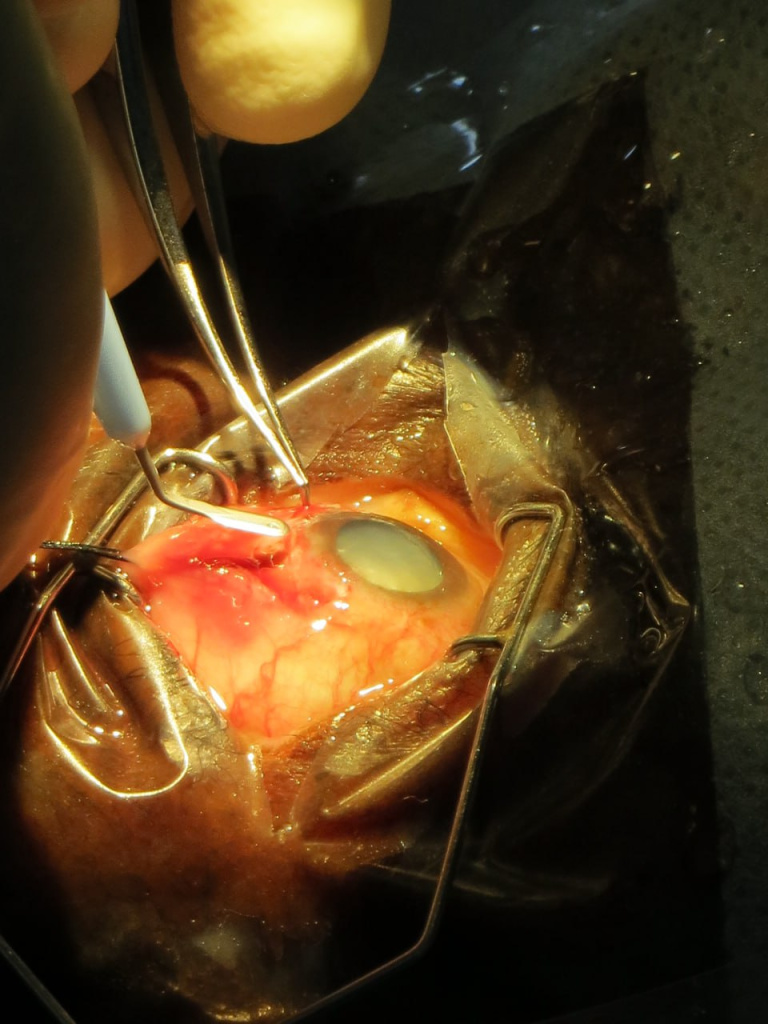
Here is how it all happened that day. My future wife was with me on my first day in the operating room and was able to take these photos. It was incredibly unusual, my heart was bursting with a thirst for new experiences, surrounded by new people, new impressions every working day. In April, my boss and later a good friend David finally agreed to teach me manual small incision cataract surgery (MSICS). Before that, I had the honor of observing his art for several months non-stop. The burning call of fearless youth… Even now, as I study phaco, it’s not as sharp or exciting as it used to be that days. Mistakes were surely made. My teacher had to correct my sclerocorneal tunnels more than once. Pay attention to the instrument table. That is exactly how much you need to effectively remove cataracts without a phaco machine and sutures.
And after the operating days, we sat together on the banks of the Zambezi River and enjoyed the sunset, not knowing that those were some of the best days of our lives.
Zambezi River, ZambiaSenanga, September 2015
Later, when I grew up and my teacher left me, I started doing independent outreach trips. This next photo is from the same town of Senanga, but already from September 2015.
Behind me are cataract patients operated on in one day. Yes, the amount of good that can be done using that limited set of instruments from the previous photos is global in both direct and figurative senses. Global ophthalmology rocks.
The guys from HelpMeSee have developed an alternative to Eyesi for manual small incision cataract surgery. Not sure if the target developing countries will have the access to it, but it’s just the beginning…
Not surprisingly, it does not provide akinesia. However, its anesthesia is sufficient for more or less comfortable surgery. It’s only obstacle is a chemisis, which is especially disturbing for novice surgeons.
Manual small incision cataract surgery (MSICS) is a gold standard for high-volume cataract services in developing countries. Since recently (with the rise of global ophthalmology concept) it has become part of the best ophthalmology training programs in the US and across the world. It is an absolutely brilliant and gentle technique, which is especially suited for premature, mature and hypermature cataracts, as well as traumatic and congenital cataracts. But one can also apply the same technique to operate on immature cataracts. Here it won’t be so fast, as the aspiration of sticky cortex will take its time with Simcoe cannula. Nevertheless, all the stages are doable.
There are differences in capsulotomy diameter, which one needs for “normal” immature cataracts (~5-6 mm) and for hypermature cataracts (up to 9-10 mm!). In mature cataracts one has to use a dye (trypan blue), but also often to carefully decompress an elevated intralenticular pressure (which often fails and leads to capsular tear and/or “argentinian flag”-style tears)! This makes capsulotomy (and capsulorhexis as one of them) in mature cataracts more complex if compared to the one in immature “transparent” cataracts.
For MSICS I personally preferred mainly a so-called “can-opener” type of capsulotomy, as it is a) easier, b) faster, and c) safer. Once I had realized these benefits, I switched to this technique almost invariably. Can-opener is best for big mature nuclei and also for Morgagnian cataracts. I am, however, aware, that can-opener is almost always not a good option for phaco. At the same time I found continuous curvilinear capsulorhexis (CCC) technique in transparent (immature) cataracts pretty easy to perform in comparison to intumescent hypermature cataracts. However, CCC is also possible by MSICS on mature cataracts. One can do it through both a tunnel or a paracentesis. A tunnel offers greater maneuverability, a paracentesis offers more stable anterior chamber.
For CCC in MSICS one can employ a) insuline syringe needle, b) Utrata forceps (gives the best control over rhexis!) and c) McPherson tying forceps. The latter is non-toothed and is a sort of improvisation, when the correct forceps is inavailable (often the case in Tropics!). In this video I depicted typical variants of CCC by mature and hypermature (and intumescent and Morgagnian!) cataracts, both uncomplicated and complicated cases. The can-opener technique is presented in two cases here and also in the other video of this channel.
* Some of the videos were screened at the earlier stage of my MSICS career. Some of the capsulotomies depicted here could have been managed better, and do not necessarily represent the best possible surgical technique. After I had bought Utrata capsulorhexis-forceps during my trip to the USA in early 2017, I never used McPherson for this purpose anymore. So, I highly recommend to purchase Utrata early in your MSICS career. The video will however be a good one for the MSICS beginners in the tropics, who often have to tackle the complex intumescent lenses with suboptimal instruments, and who still have the right to do mistakes 🙂 I would anyways appreciate your (also critical) comments.
Those of you, who just start with MSICS – Keep it up!