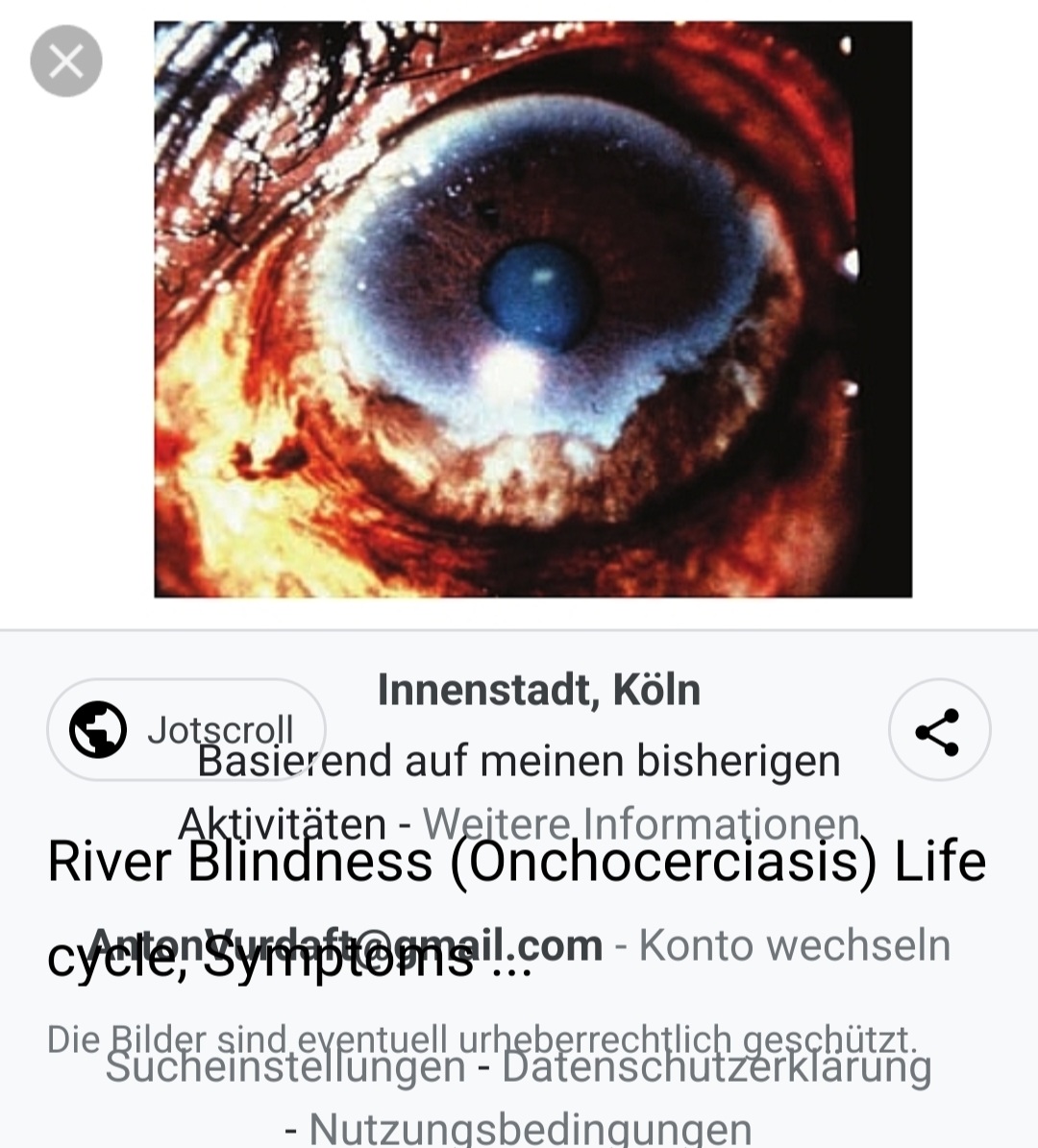
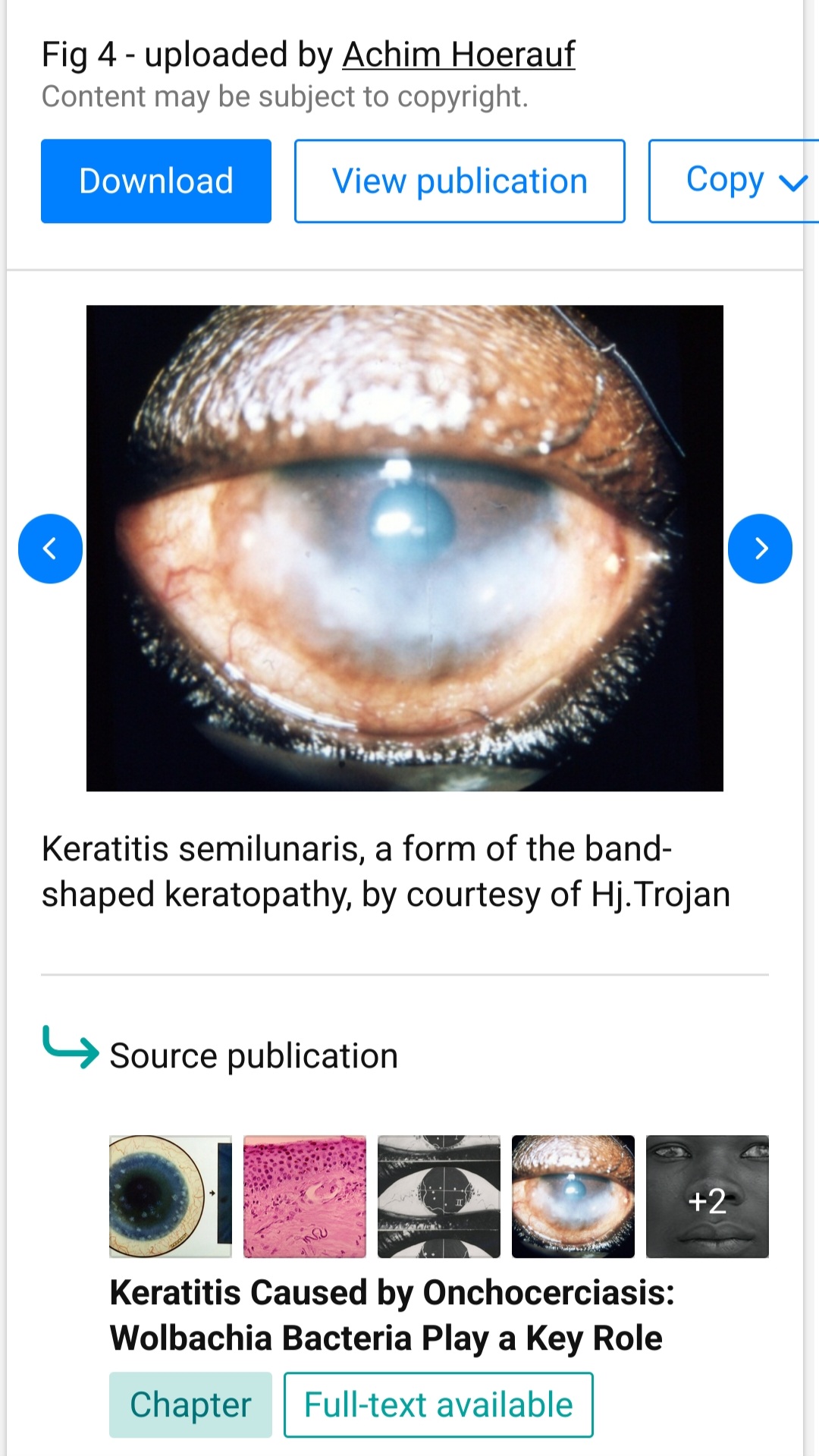
“The characteristic facial expression of the onchocerciasis patients is also based on the interstitial keratitis, which prefers a horizontal axis and creates a vertical positioned ovular bow in the ribbon shaped degeneration of the cornea”. (c) Dr. Guido Kluxen’s excellent reasearch book “Dr. Jean Hissette’s Research Expeditions to Elucidate River Blindness”, 2011
I think I had never seen onchocerciasis patients in Zambia. Although onchocerciasis is not endemic there, one sees daily unclear corneal opacities as a result of various keratitides or uveitides. Some patients travel from Angola, Namibia and Congo. The latter should still be endemic… So I decided to google these corneas, as the description is not too descriptive.