Senanga town, Western Province of Zambia. April 2014.



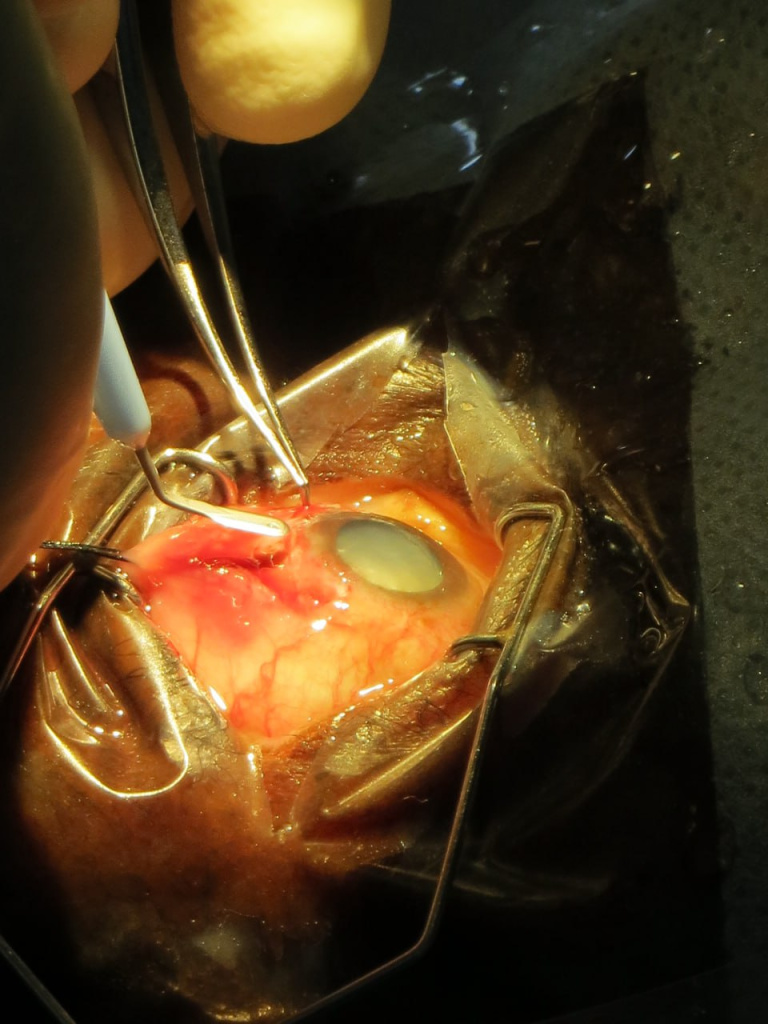
Here is how it all happened that day. My future wife was with me on my first day in the operating room and was able to take these photos. It was incredibly unusual, my heart was bursting with a thirst for new experiences, surrounded by new people, new impressions every working day. In April, my boss and later a good friend David finally agreed to teach me manual small incision cataract surgery (MSICS). Before that, I had the honor of observing his art for several months non-stop. The burning call of fearless youth… Even now, as I study phaco, it’s not as sharp or exciting as it used to be that days.
Mistakes were surely made. My teacher had to correct my sclerocorneal tunnels more than once.
Pay attention to the instrument table. That is exactly how much you need to effectively remove cataracts without a phaco machine and sutures.
And after the operating days, we sat together on the banks of the Zambezi River and enjoyed the sunset, not knowing that those were some of the best days of our lives.




Later, when I grew up and my teacher left me, I started doing independent outreach trips. This next photo is from the same town of Senanga, but already from September 2015.
Behind me are cataract patients operated on in one day. Yes, the amount of good that can be done using that limited set of instruments from the previous photos is global in both direct and figurative senses. Global ophthalmology rocks.