![]() It is sad to see a very young person going needlessly blind. This is a case of bilateral advanced stage juvenile glaucoma in young 16 y.o. lady. She had bilateral deepest cupping of 1,0 and 6/60 vision in one eye and finger counts at 3 m in the other. Her intraocular pressures were, as it is common here and especially in young persons, – slightly below 50 mm Hg in one eye and 55 mm Hg in the other eye.
It is sad to see a very young person going needlessly blind. This is a case of bilateral advanced stage juvenile glaucoma in young 16 y.o. lady. She had bilateral deepest cupping of 1,0 and 6/60 vision in one eye and finger counts at 3 m in the other. Her intraocular pressures were, as it is common here and especially in young persons, – slightly below 50 mm Hg in one eye and 55 mm Hg in the other eye.
The problem of glaucoma in Africa is described nicely and in details elsewhere: https://www.iapb.org/blog/my-challenges-managing-glaucoma-sub-saharan-africa, https://www.ncbi.nlm.nih.gov/pubmed/19225348. My few cents will be like this (in order of relevance):
- Lack of early recognition among the patients
- Lack of IOP and disks screening among even trained mid-level ophthalmic staff
- Poverty, leading to huge delays to a hospital visit
- Poverty, leading to inability to buy medications for chronic disease
- Unavailability of fency eye drops (only timolol is available in most of rural places, and it’s value in IOP 50 mm Hg is from limited to none)
- Lack of follow-ups, leading to unnecessary failure of trabeculectomies
Each of those makes majority of patients with glaucoma present in advanced stages (rarely amenable to medications).
I opted bilateral trabeculectomy with 5-fluorouracil in this case (however, in ideal circumstances I would preferr mitomycin – it is stated to be more effective in studies). She underwent uneventful surgeries for both eyes (one week apart). Right eye (the worse eye), however, showed persistent leakage from fornix-based bleb, and had to be sutured additionally after a week postop. Both eyes dropped the IOPs to mid teens, and the girl’s parents were counselled properly on very important follow-ups during next few months. Failure of trabeculectomy is common first 6 months after the surgery.
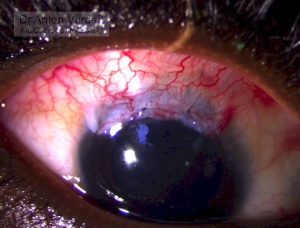
Right eye: Bleb additionally sutured to close leakage. I acknowledge, that this is not the ideal way to close leaking bleb, and will release this sutures upon ten days.

Left eye: fornix based diffuse bleb
P.S. I am still not sure on what is the best practice in trabeculectomy in african population regarding the tenon’s capsule. It can be either excised a little, or just undermined, or even sutured to the limbus below the conjunctiva. There were no RCTs on that, and that’s quite important: I feel the chances are higher for the bleb to become cystic if tenon’s was excessively excised.