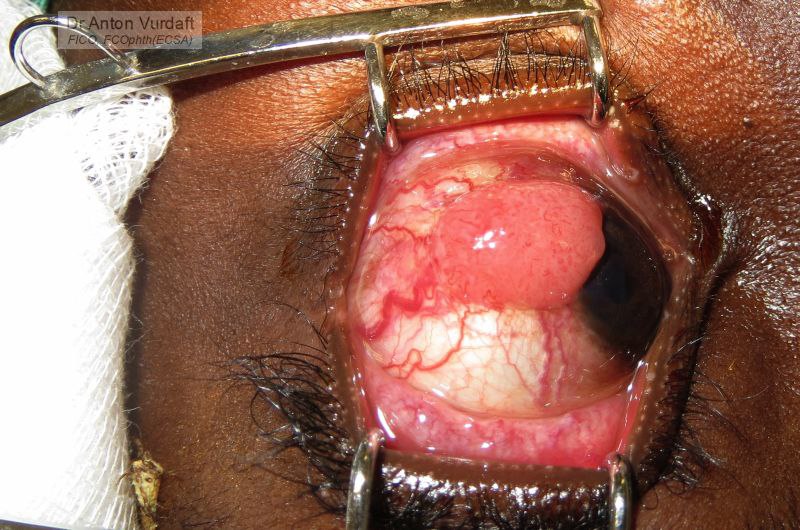
![]() EN: A case of September 2016. Squamous cell carcinoma of conjunctiva (SCC). A young male patient had recently found out his positive HIV status. This SCC is yet presumably non-invasive to the sclera. This tumor was unresponsive to three on-off cycles of 5-fluorouracyl (5-FU) eye drops. The risk of recurrence after simple excision with antimetabolites is relatively high.
EN: A case of September 2016. Squamous cell carcinoma of conjunctiva (SCC). A young male patient had recently found out his positive HIV status. This SCC is yet presumably non-invasive to the sclera. This tumor was unresponsive to three on-off cycles of 5-fluorouracyl (5-FU) eye drops. The risk of recurrence after simple excision with antimetabolites is relatively high.
Of interest: the eye removal (enucleation) was not indicated. The tumor was excised (no-touch technique) with application of 5-FU. Superficial sclerectomy is also a good additional measure to avoid recurrence in cases suggestive of sclera invasion. However in this case an additional cryotherapy was planned, but failed due to machine failure. The patient was referred for the cryo into the capital city.
Also of interest: it is not wise to cover the resultant defect with conjunctiva, there is a risk of recurrence, which we can thus miss. Nevertheless, the option of amniotic membrane coverage is described in the literature, and I witnessed this technique in the USA.
The chances for exenteration in future in African setup are relatively high! The patients with the eyes, which can see 1,0, rarely allow eye amputation, thus receiving often a super-huge tumors, amenable only to exenteration!
A similar case was already presented in the Atlas (see the link below).
![]() RU: Случай от сентября 2016 г. Плоскоклеточный рак конъюнктивы. Молодой пациент, недавно узнавший о своём положительном статусе по ВИЧ. Плоскоклеточный рак, предположительно пока без склеральной инвазии. Этой опухоли не помогли три цикла химиоредукции с 5-фторурацилом. Крайне высокие риски на рецидив, даже с применением антиметаболитов.
RU: Случай от сентября 2016 г. Плоскоклеточный рак конъюнктивы. Молодой пациент, недавно узнавший о своём положительном статусе по ВИЧ. Плоскоклеточный рак, предположительно пока без склеральной инвазии. Этой опухоли не помогли три цикла химиоредукции с 5-фторурацилом. Крайне высокие риски на рецидив, даже с применением антиметаболитов.
Ложе после удаления опухоли конъюнктивой не покрывается: это чревато пропуском рецидивов. Тем не менее, в США я наблюдал покрытие ложа амнионом. Такое описано в литературе и часто практикуется.
Тактика на момент лечения не включала в себя удаление глаза! Эта опухоль была иссечена. Недостаточно глубоко.. Планировал крио, но вышли проблемы с газом. При отсутствии крио шансы на повторный рост были очень высокие: такие опухоли требуют помимо аппликации антиметаболитов и некоторый объём склерэктомии (чего в данном случае не было сделано). Пациент был направлен на криолечение в столицу. Шансы на то, что закончиться это могло, тем не менее, не энуклеацией – экзентерацией, – относительно немалые, по простой причине: пациенты, особенно с рецидивами, и особенно со зрением единица – не готовы к удалению глаза, запуская рост опухоли до крайних размеров.
Аналогичный случай с похожей опухолью уже представлен в атласе: Conjunctival Squamous Cell Carcinoma.
Advanced OSSN
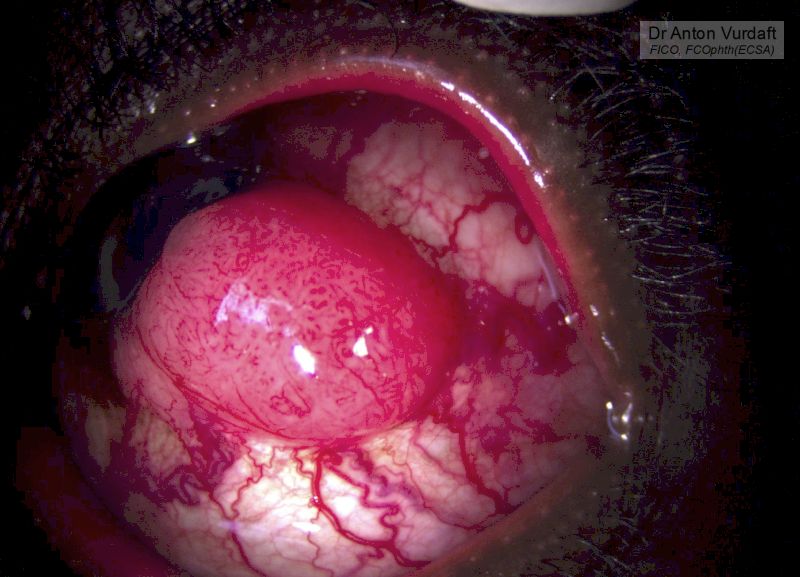
Advanced OSSN
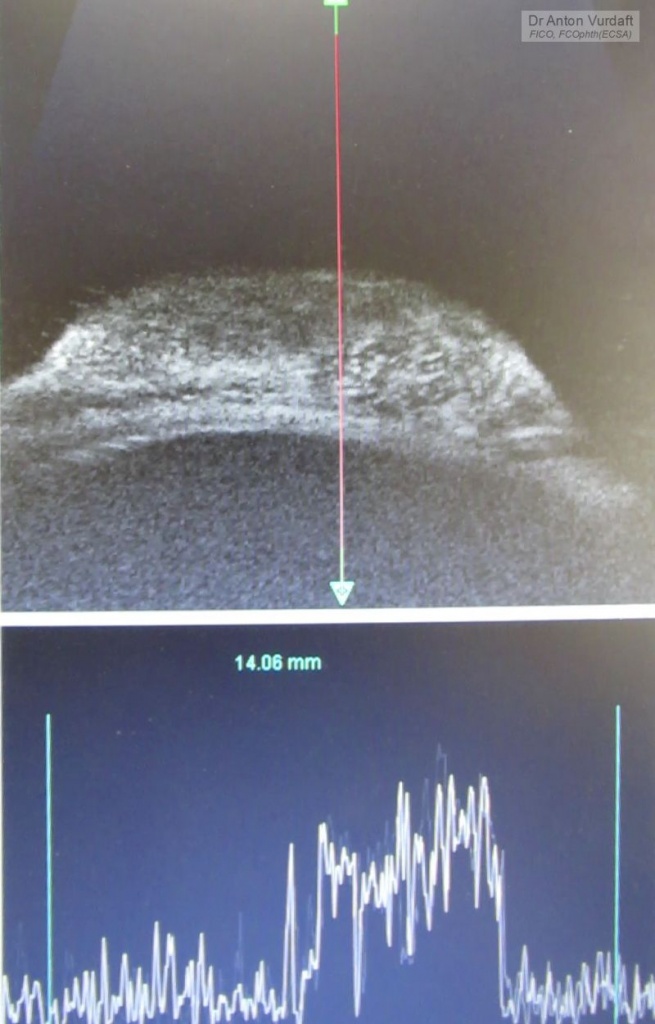
Advanced OSSN ultrasound biomicroscopy
