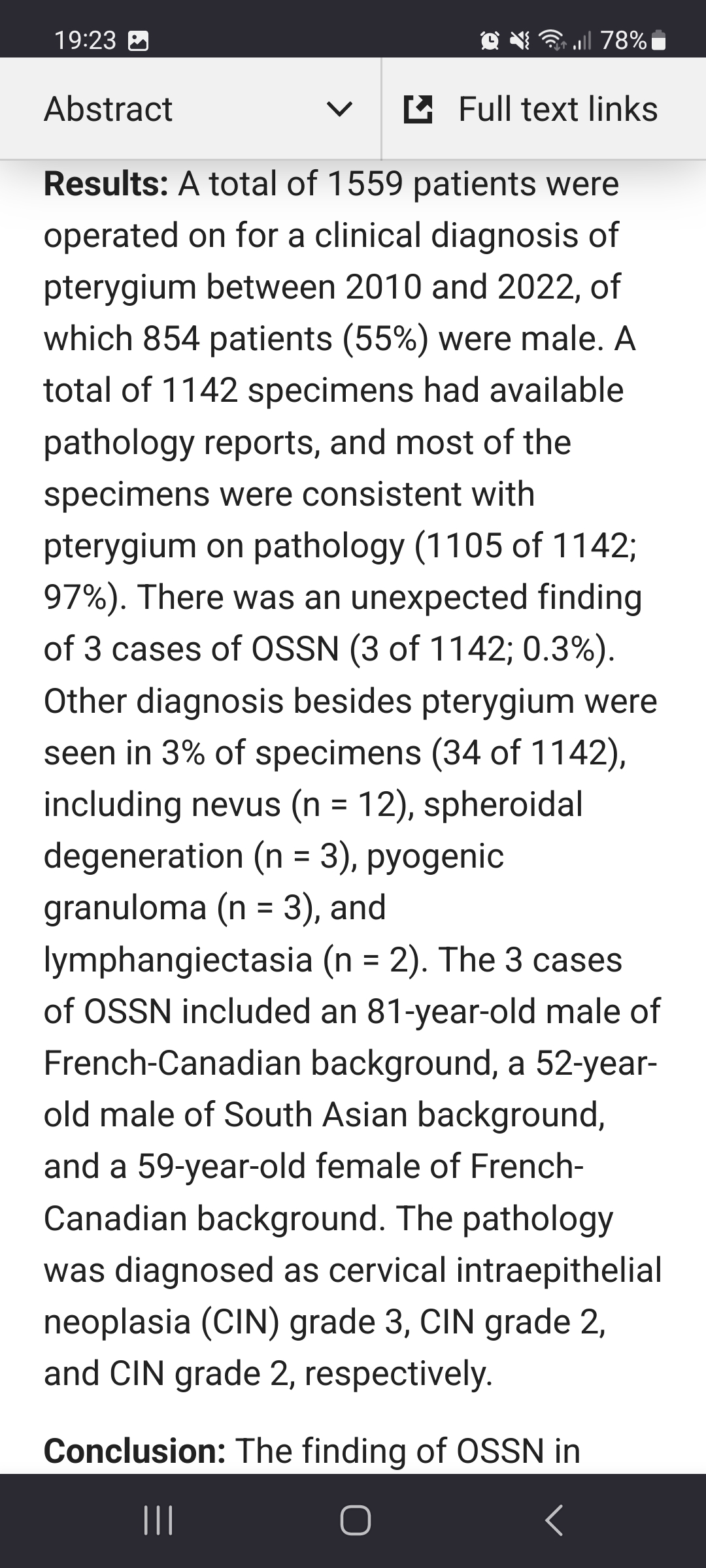
There’s a new study from Canada, where they found, that around 3% of excised pterygia are appeared to be pcular surface squamous neopleasia histologically. In endemic regions of Africa this percent schould be much higher.
Eye Diseases Seen in Sub-Saharan Africa
There’s a new study from Canada, where they found, that around 3% of excised pterygia are appeared to be pcular surface squamous neopleasia histologically. In endemic regions of Africa this percent schould be much higher.
In our Setup in Zambia one rule which we used to have was: as soon as OSSN involves a caruncle or conjunctival fornices, the eye (no matter how good it could see) should be planned to exenteration or at least extended enucleation). I used to not to question this practice in the abscence of MRI at hand.
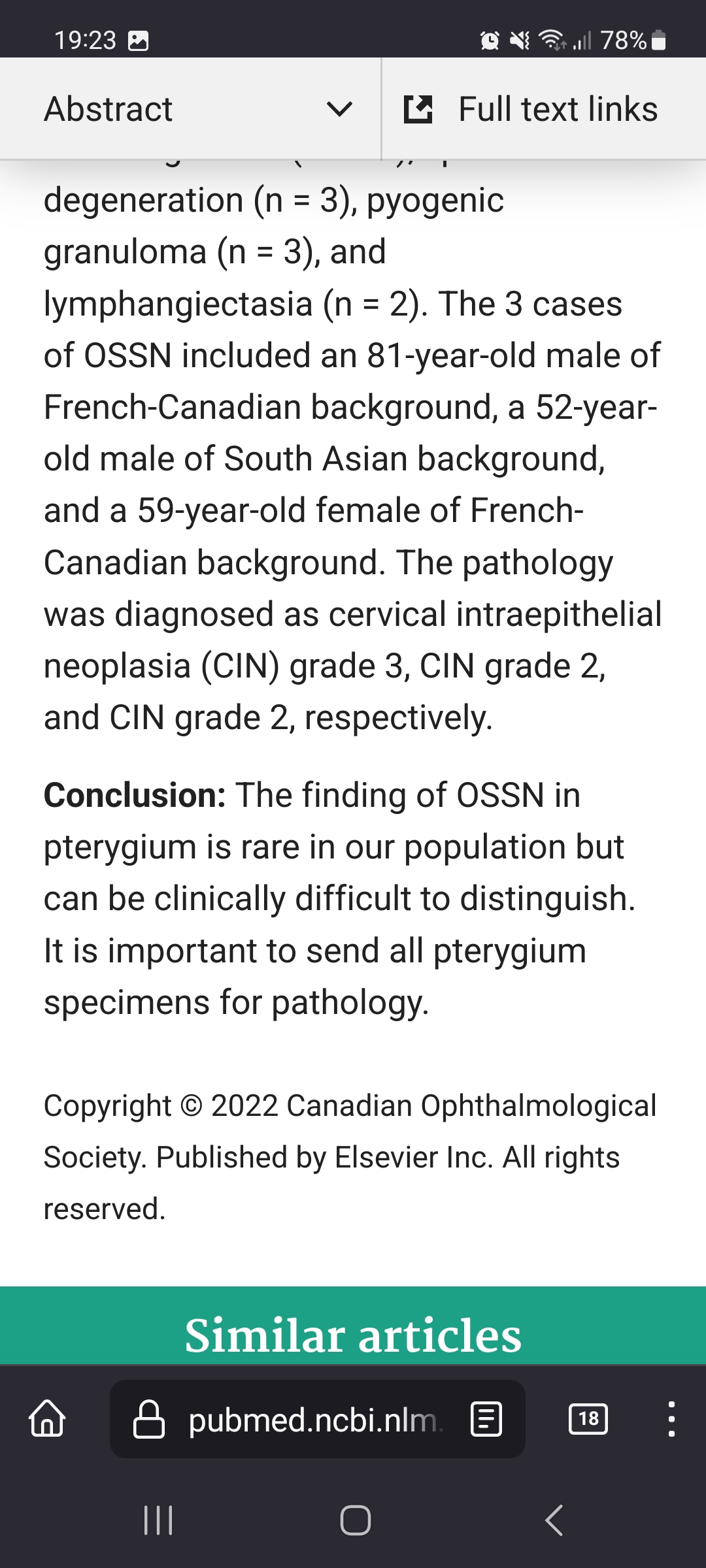
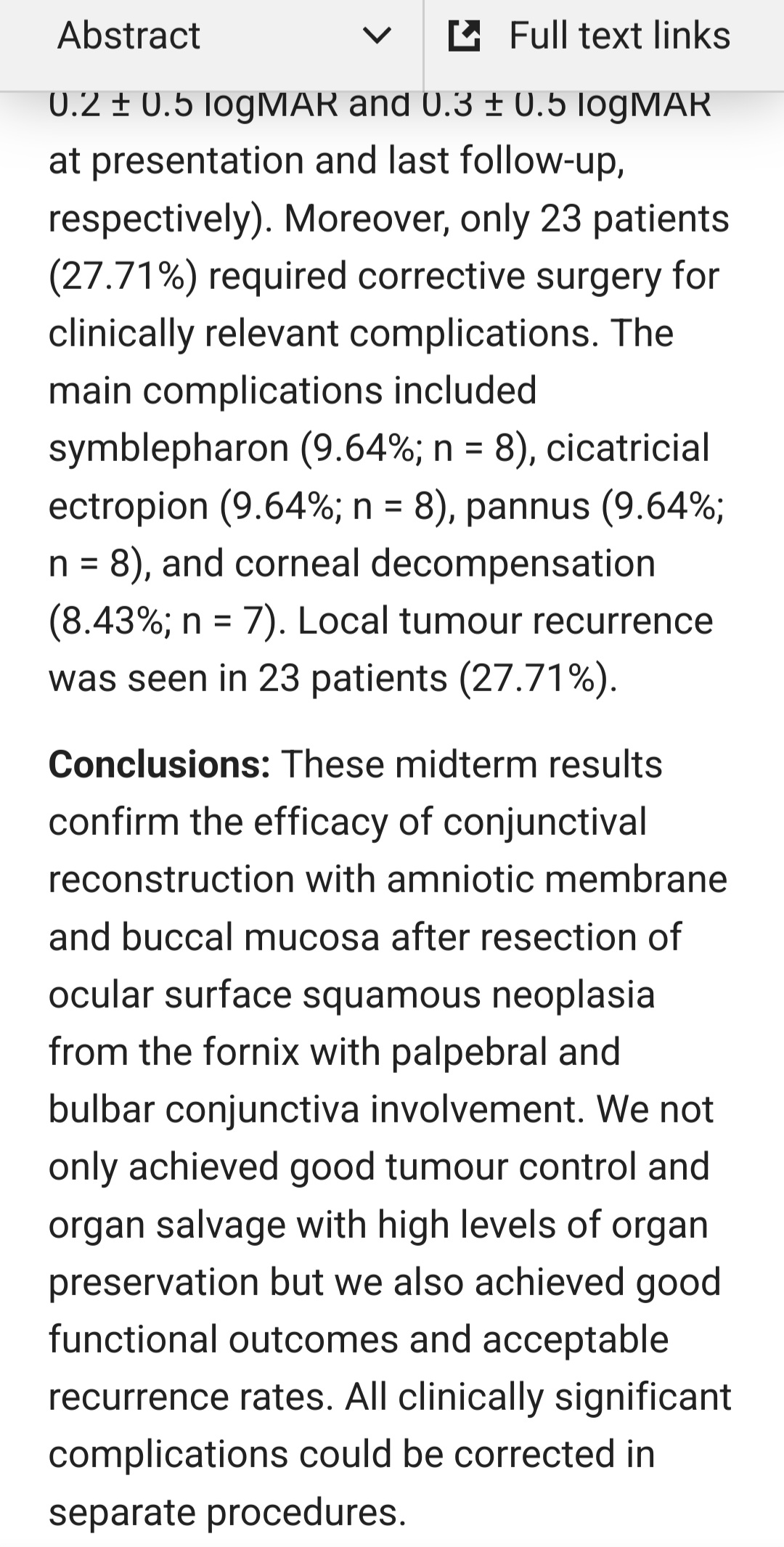
However, fellows from Duisburg (Germany) proved that an excision of forniceal OSSN can still be good compensated with buccal or amniotic mucous membrames. And recurrencies of ~30%. Which is actually not bad considering the mutilating alternative. A food for thought. https://pubmed.ncbi.nlm.nih.gov/35940212/
In the western world it is rare, to miss an OSSN and excise it as pterigium without no-touch technique etc. In one retrospective study from the US it was only in 0,3% of all cases of pterygium excision.
In tropical Africa, such cases are much more often. And vice versa, it is also commom to see a very suspective pterygium, that upon pathology proves to be benign… See this: Case 1 and Case 2
In this blog one may find lots of pictures of OSSN. Finally we got some science for that!
Clinical and Pathologic Presentation of Primary Ocular Surface Tumors among Zambians
Peter Julius et al. Ocul Oncol Pathol. 2021 Mar;7(2):108-120.
doi: 10.1159/000511610. Epub 2021 Jan 21.
Authors
Peter Julius 1 , Stepfanie N Siyumbwa 1 , Phyllis Moonga 2 , Fred Maate 1 , Trevor Kaile 1 , Guobin Kang 3 , John T West 4 , Charles Wood 3 , Peter C Angeletti 3
1 Department of Pathology and Microbiology, School of Medicine, Lusaka, Zambia.
2 University Teaching Hospital, Eye Hospital, Lusaka, Zambia.
3 Nebraska Center for Virology and the School of Biological Sciences, University of Nebraska-Lincoln, Lincoln, Nebraska, USA.
4 Nebraska Center for Virology and the Department of Biochemistry, University of Nebraska-Lincoln, Lincoln, Nebraska, USA.
PMID: 33869164
PMCID: PMC8024974 (available on 2022-03-01)
DOI: 10.1159/000511610
Aim: This study aimed to characterize the clinical and pathologic presentation of ocular surface tumors (OSTs) and to more precisely differentiate the grades of ocular surface squamous neoplasia (OSSN) and benign lesions among Zambians.
Methods: Two-hundred sixty-five Zambian patients presenting with ocular surface growths, suspicious for OSSN, were recruited between November 2017 and November 2019 to a cross-sectional study to investigate their lesions. Sociodemographic data were collected, HIV infection status and vision tests were performed, and lesions were measured and documented. Lesions >2 mm in diameter were excised and sent for pathology analysis. In addition to the biopsies, tears, blood, and buccal swabs were collected. CD4+ T-cell counts were measured by flow cytometry. Lesions were classified according to the WHO guidelines. χ2 and bivariate correlations were used to analyze variable associations and strengths with phi/Cramer’s V and correlation coefficients, respectively. Binary logistics was used to adjust for covariance.
Results: In this study, 68.3% of the participants were found to be HIV positive. The most frequent diagnoses were invasive OSSN (45.3%), preinvasive OSSN (29.1%), and pterygium (22.6%). Invasive OSSN comprised keratinizing squamous cell carcinoma (SCC) (87.5%), basaloid SCC (3.3%), and spindle cell carcinoma (3.3%). Unusual carcinomas, not described previously, included hybrid SCC (5.0%) and acantholytic SCC (0.8%). Invasive OSSN had advanced tumor (T3/T4) staging (93.3%) at diagnosis. Lymphadenopathy was rare (2.3%), and metastasis was absent. Patients were mostly female (59.2%). Median age was 36 (interquartile ranges 33-41) years (ranges 18-81). Patients with invasive OSSN were more likely to present with pain (p = 0.007), redness (p = 0.034), excessive tearing (p = 0.0001), discharge (p = 0.011), bleeding (p = 0.007), reduced vision (p = 0.0001), fungating lesion (p = 0.001), and blindness (p = 0.005); location at temporal limbus (p = 0.0001), inferior limbus (p = 0.0001), or circumlimbal (p = 0.001); and extension to cornea (p = 0.006) and forniceal palpebral conjunctiva (p = 0.001). Invasive OSSN was associated with any smoking habit and alcohol consumption (p = 0.04 and 0.03, respectively). HIV positivity was strongly associated with OSSN (74.6% OSSN vs. 49.3% benign lesions; p = 0.0001; phi: 0.237 [p = 0.0001]).
Conclusion: OSTs are very common in Zambia and are strongly associated with HIV coinfection. Patients with OSSN were more likely to be HIV positive than those with pterygia. Despite the commonality of OSTs in sub-Saharan Africa, these cancers have historically been poorly characterized