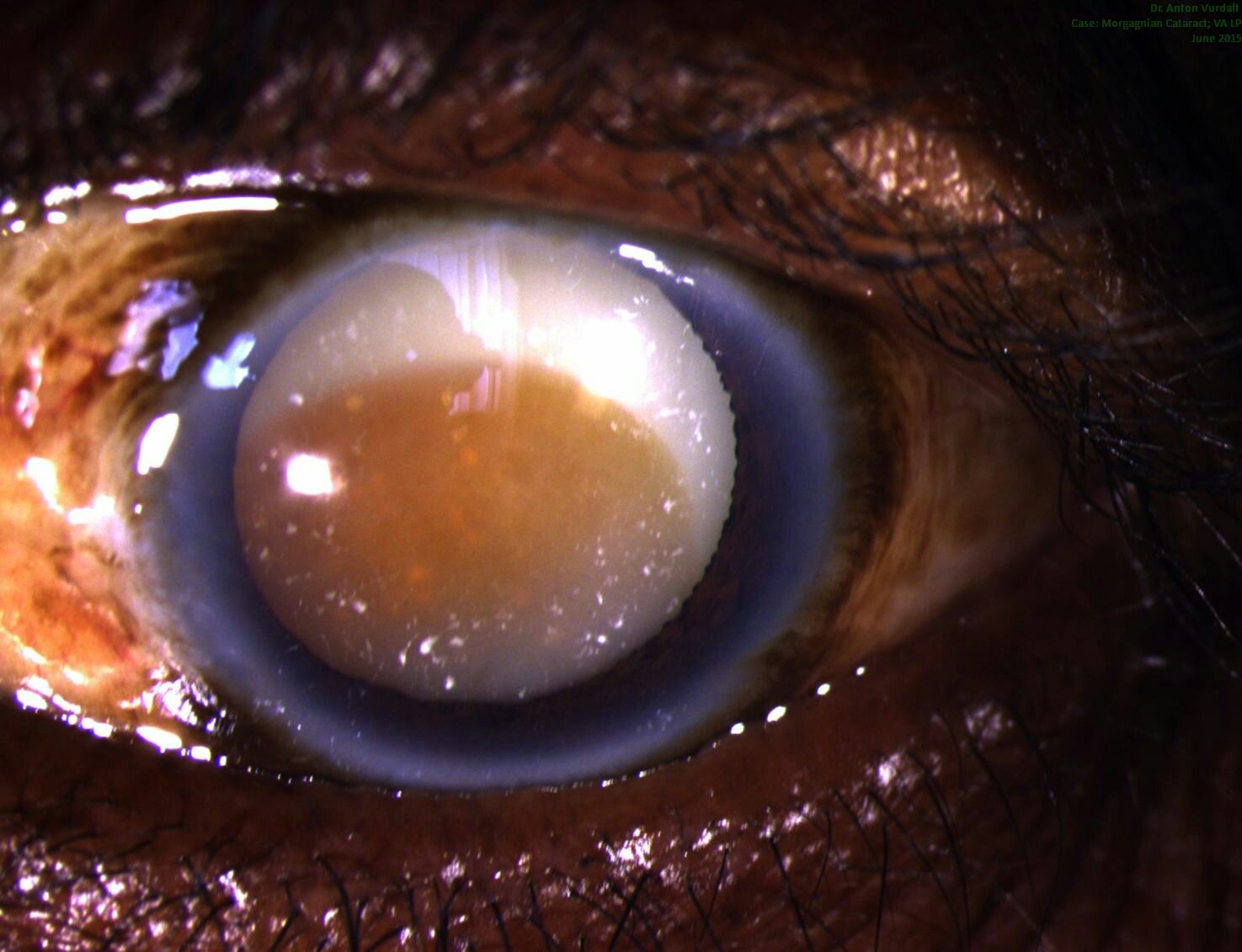
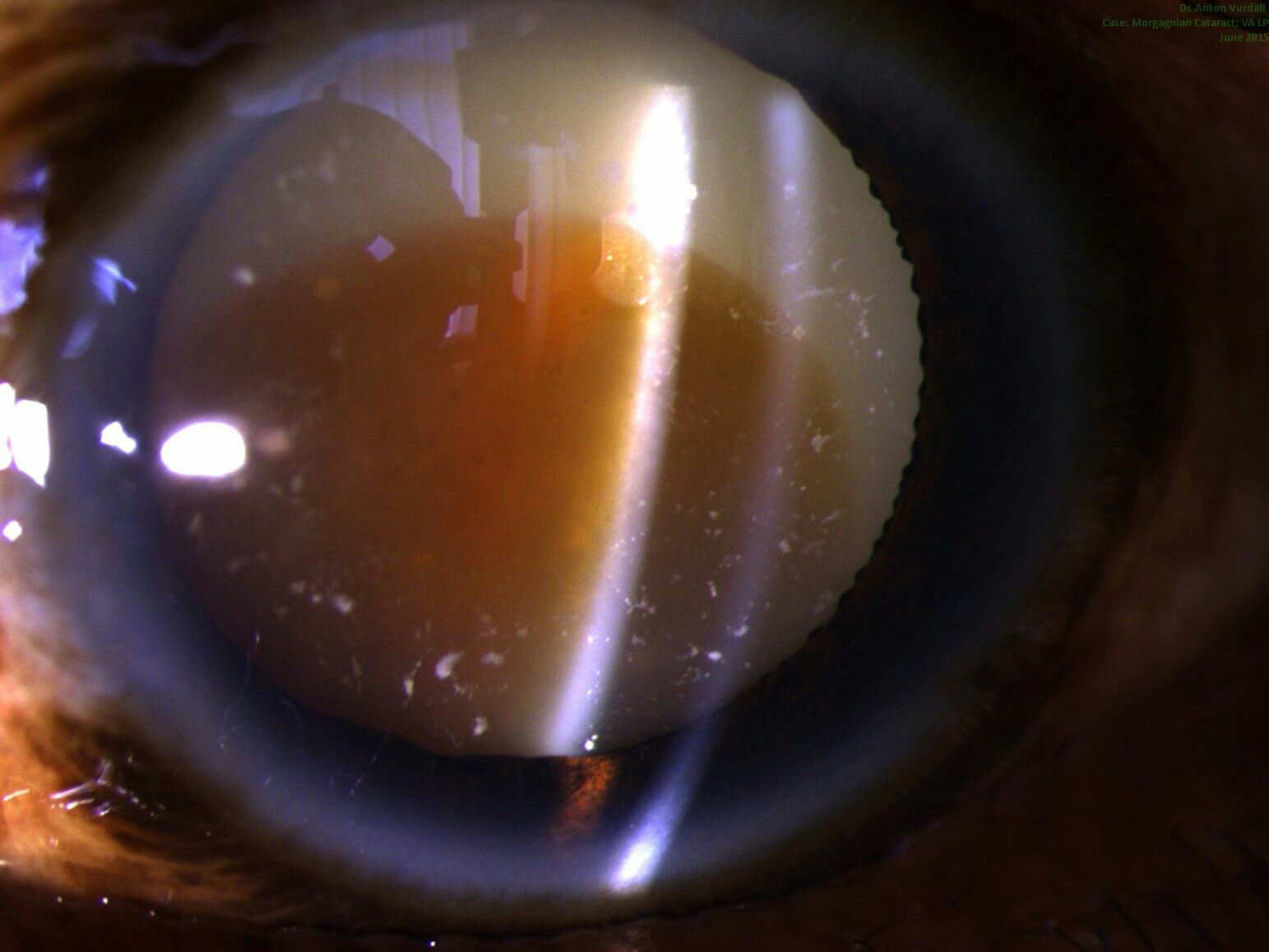
Zuweilen soll das Trübwerden des Morgagnischen Liquor den Staar, welcher alsdann Morgagnischer Staar (Cataracta Morgagniana s. intertitialis) genannt wird, bedingen; dieses Uebel wird aber selten beobachtet, da Trübungen des Morgagnischen Dunstes schnell die Verdunklungen der Linse bedingen.
Quelle: Beck, Handbuch der Augenheilkunde (1823), S. 258-259
Dr. Jean Hissette’s cataract surgery in Kasai in the Belgian Congo, 1930
Photo from Dr. Guido Kluxen’s excellent reasearch book “Dr. Jean Hissette’s Research Expeditions to Elucidate River Blindness”, 2011
Interestingly, Dr. Hissette performed his cataract OPs using large conjunctival peritomies and additionally – iridectomies. Many surgeries were complicated with synechias, which were typicall for onchocerciasis induced uveitis.
I found interesting as well, how the doctor treated assistance during these OPs: “I did the surgeries without assistance, as I believe that if you do not have adequate assistance, it is better to operate without any”. May be often the case in the tropical setup.
Dr. Jean Hissette’s cataract surgery in Kasai in the Belgian Congo, 1930 (Photo from Dr. Guido Kluxen’s excellent reasearch book “Dr. Jean Hissette’s Research Expeditions to Elucidate River Blindness”, 2011)
Manual small incision cataract surgery (MSICS) is a gold standard for high-volume cataract services in developing countries. Since recently (with the rise of global ophthalmology concept) it has become part of the best ophthalmology training programs in the US and across the world. It is an absolutely brilliant and gentle technique, which is especially suited for premature, mature and hypermature cataracts, as well as traumatic and congenital cataracts. But one can also apply the same technique to operate on immature cataracts. Here it won’t be so fast, as the aspiration of sticky cortex will take its time with Simcoe cannula. Nevertheless, all the stages are doable.
There are differences in capsulotomy diameter, which one needs for “normal” immature cataracts (~5-6 mm) and for hypermature cataracts (up to 9-10 mm!). In mature cataracts one has to use a dye (trypan blue), but also often to carefully decompress an elevated intralenticular pressure (which often fails and leads to capsular tear and/or “argentinian flag”-style tears)! This makes capsulotomy (and capsulorhexis as one of them) in mature cataracts more complex if compared to the one in immature “transparent” cataracts.
For MSICS I personally preferred mainly a so-called “can-opener” type of capsulotomy, as it is a) easier, b) faster, and c) safer. Once I had realized these benefits, I switched to this technique almost invariably. Can-opener is best for big mature nuclei and also for Morgagnian cataracts. I am, however, aware, that can-opener is almost always not a good option for phaco. At the same time I found continuous curvilinear capsulorhexis (CCC) technique in transparent (immature) cataracts pretty easy to perform in comparison to intumescent hypermature cataracts. However, CCC is also possible by MSICS on mature cataracts. One can do it through both a tunnel or a paracentesis. A tunnel offers greater maneuverability, a paracentesis offers more stable anterior chamber.
For CCC in MSICS one can employ a) insuline syringe needle, b) Utrata forceps (gives the best control over rhexis!) and c) McPherson tying forceps. The latter is non-toothed and is a sort of improvisation, when the correct forceps is inavailable (often the case in Tropics!). In this video I depicted typical variants of CCC by mature and hypermature (and intumescent and Morgagnian!) cataracts, both uncomplicated and complicated cases. The can-opener technique is presented in two cases here and also in the other video of this channel.
* Some of the videos were screened at the earlier stage of my MSICS career. Some of the capsulotomies depicted here could have been managed better, and do not necessarily represent the best possible surgical technique. After I had bought Utrata capsulorhexis-forceps during my trip to the USA in early 2017, I never used McPherson for this purpose anymore. So, I highly recommend to purchase Utrata early in your MSICS career. The video will however be a good one for the MSICS beginners in the tropics, who often have to tackle the complex intumescent lenses with suboptimal instruments, and who still have the right to do mistakes 🙂 I would anyways appreciate your (also critical) comments.
Those of you, who just start with MSICS – Keep it up!
There is a good retrospective study from Nigeria showing that trends to operate only the advanced stages of cataract persist in Sub-Saharan Africa. That means that a patient with cataract would typically get his cataract removed only when they are blind (i.e. 0,05 or 3/60 and beliw, HM, LP etc.). In this context it is important to remember, that MSICS technique of cataract surgery is safer in premature and matute stages of cataract, which can influence the willingness to operate among surgeons.
Ther Adv Ophthalmol. 2019 Jan-Dec; 11: 2515841419886451.
Published online 2019 Nov 13. doi: 10.1177/2515841419886451
PMCID: PMC6854760
PMID: 31763621 Preoperative visual acuity of cataract patients at a tertiary hospital in sub-Saharan Africa: a 10-year review
Mary O. Ugalahi, Obioma C. Uchendu, and Linda O. Ugalahi
Mary O. Ugalahi, Department of Ophthalmology, College of Medicine, University of Ibadan and University College Hospital, Ibadan, Ibadan, Nigeria; Department of Ophthalmology, College of Medicine, University of Ibadan and University College Hospital, 200212 Ibadan, Ibadan, Nigeria;
Purpose:
To determine the preoperative visual acuity of cataract patients over a 10-year period in a tertiary facility as a means of auditing the cataract surgical services.
Methods:
A retrospective study of patients with age-related cataracts who had cataract surgery performed between January 2007 and December 2016 at the University College Hospital, Ibadan. Systematic random sampling and probability proportionate to size were used to recruit a representative sample. Information on sociodemographic characteristics, preoperative visual acuity, ocular and systemic comorbidities were retrieved and analysed.
Results:
Of the 499 patients studied, males were 268 (53.7%) and their mean age was 67.69 (±9.51) years. The predominant visual acuity was hand motion 184 (36.9%) and yearly mean preoperative visual acuity was in the range of 0.0037–0.04 decimal.
Conclusion:
The mean preoperative visual acuity of patients in this facility did not change over the 10-year study period. Mean value of preoperative visual acuity remained within the range of blindness and did not improve over the decade. This could either be a reflection of visual impairment at which our patients seek care or an indication of the range of visual acuities at which surgeons are willing to offer cataract surgery in our environment. This trend has negative implications on the burden of cataract blindness as it reflects poor coverage of surgery for other levels of visual impairment due to cataract.