![]() This is a relatively young lady (27yo), who presented with bilateral decrease of vision since one month ago. She is of those patients, whose diagnosis is clear right at the doorstep: big eyes, staring gaze immediately suggest thyroid problems. She claims no history of headaches, nausea or vomitting. She had episodes of pains in medial canthi area (?carunculitis), but no gross dry eye symptoms.
This is a relatively young lady (27yo), who presented with bilateral decrease of vision since one month ago. She is of those patients, whose diagnosis is clear right at the doorstep: big eyes, staring gaze immediately suggest thyroid problems. She claims no history of headaches, nausea or vomitting. She had episodes of pains in medial canthi area (?carunculitis), but no gross dry eye symptoms.
Her vision, she confirms, is lower in the right eye (6/36, vs 6/6 in LE).
There is no gross proptosis (probably mild proptosis is there, but I do not have Hertel’s). Her eyelids exam reveals scleral show both above and below limbus, but this “show” is dynamic, increasing when she concentrates on something. This is typical for thyroid disease (Kocher’s sign). She shows no lid lag, no lagophthalmos, no static upper lid retraction, her MRD distance is normal on static exam, but lid fissures are 14 and 13 mm, which is a slight oversize. Her upper lids function is normal. Her lower lid shows mild retraction in static relaxed position (1-2 mm of scleral show).
Her extraocular motility (surprisingly!) is unrestricted, full and causing no diplopia in any of the gazes.
Her anterios segments were anremarkable (and RAPD was not assessed – she was already dilated to that time).
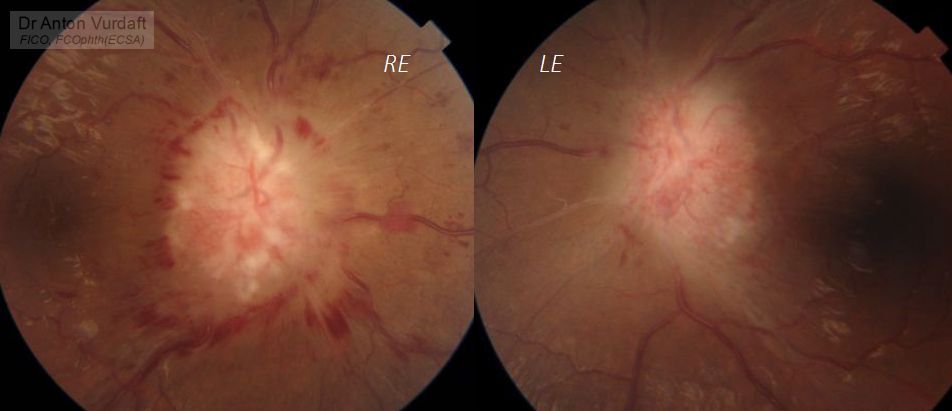
Her fundus picture showed gross optic disc swelling both eyes (right eye more), causing some intraretinal hemorrhages and retinal folds around the disc. Moderate veins tortuosity.
Her color vision appeared to be disturbed moderately. Her vision fields were severely impaired (surprisingly, left eye was more involved), and are depicted in attachment.
Her IOPs were normal.
She has no other symptoms of possible dysthyroidism apart from slight hands tremor.
Despite an absence of gross restrictive myopathy, my tentative diagnosis would by thyroid eye disease, compressive optic neuropathy.
Due to severe optic nerve involvement I would opt in urgent intravenous steroid therapy (methylprednisolone 500 mg weekly for 6 weeks, followed by 250 mg weekly for another 6 days, or dexamethasone in equivalent doses). Hopefuly, this will restore some part of vision, and give me time for complete evaluation, including MRI of the orbits and brain, thyroid tests (T3, T4, TSH, TSI). I would control her co-existing hypertension, possile glucose issues, monitor her for possible side effects after initiation of steroids (especially for HTN). She claims no smoking.
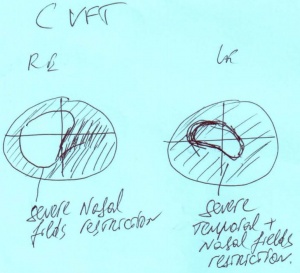
Visual field defects in confrontational visual field test
thyroid eye disease compressive optic neuropathy
I found it strange though, that possible compressive optic neuropathy in presumed thyroid eye disease is not accompanied by any gross restrictive myopathy, and am in consult with thyroid eye disease specialists.